

Abstract
Background: In the phase 3 TOWER study, patients with relapsed or refractory (r/r) Philadelphia chromosome-negative (Ph-) B-cell precursor (BCP) acute lymphoblastic leukemia (ALL) who received bispecific T-cell engager (BiTE®) antibody construct blinatumomab had improved overall survival (OS; median, 7.7 vs 4.0 months; P=0.01;) and health-related quality of life (HRQoL) compared with those who received standard of care (SOC) chemotherapy (Kantarjian H, et al. N Engl J Med. 2017;376:836-847; Topp MS, et al. Blood. 2018;131:2906-2914). In this subgroup analysis of TOWER, we assessed the HRQoL between patients with low versus high baseline disease burden (low versus high bone marrow blast levels) who received blinatumomab or SOC chemotherapy.
Methods: Patients (N=405) with r/r Ph- BCP ALL were randomized 2:1 to receive 2 cycles of induction blinatumomab by continuous intravenous infusion (n=271) or SOC (n=134). Those in remission could receive up to 3 consolidation cycles; 12 months of maintenance was allowed for those who received up to 3 consolidation cycles and had bone marrow response. HRQoL was assessed using the EORTC QLQ-C30 Questionnaire on days 1 (baseline), 8, and 15; on day 29 of cycle 1; days 1, 15, and 29 of consolidation; and at the safety follow-up. The questionnaire included 1 global health status scale, 5 functioning scales, 3 symptom scales, and 6 single-symptom items. For global health status and functioning scales, a higher score indicates better HRQoL; for symptom scales/items, a lower score indicates better HRQoL. A 10-point change was viewed as the minimum clinically important difference in EORTC QLQ-C30 (Zikos E, et al. EORTC. 2016). HRQoL was assessed in patient subgroups by screening the bone marrow aspirates for low blast levels (<50% blasts) versus high blast levels (≥50% blasts). Although blast count was not a randomization stratification factor in TOWER, baseline HRQoL values were assessed for blinatumomab versus SOC in both subgroups; in the high blasts group, for blinatumomab versus SOC, the only differences were cognitive functioning and constipation scores, which were significantly higher, and for the diarrhea score, which was significantly lower. Between the subgroups, only physical functioning was significantly different (higher in the high blasts group). Analyses included patients with baseline and ≥1 postbaseline result of any multi-item scale or single-item measure. Mean change from baseline in scores for each scale/item were summarized for cycle 1. Time to deterioration (TTD) analyses assessed the treatment effect based on timing from the initiation of treatment to a 10-point deterioration from baseline.
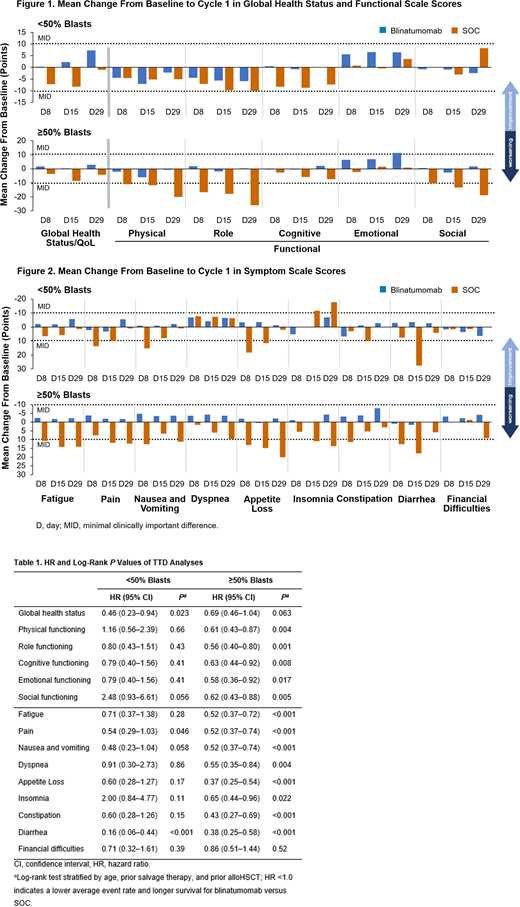
Results: In total, 342 patients (blinatumomab, n=247; SOC, n=95) had ≥1 HRQoL result: low blasts, n=87 (blinatumomab, n=64; SOC, n=23); high blasts, n=255 (blinatumomab, n=183; SOC, n=72). The EORTC QLQ-C30 analysis set included all randomized subjects with a nonmissing baseline result and at least 1 nonmissing post-baseline result of any EORTC QLQ-C30 scale/item. There was no statistically significant difference in baseline HRQoL scores between the high and low blasts groups; however, the high blasts group had worse HRQoL overall. Baseline HRQoL scores were also similar between blinatumomab arm and SOC arm for each group. Global health status was improved by blinatumomab regardless of baseline blast level; however, this effect was somewhat greater in the low blasts group. When the function scores worsened, the extent of worsening was almost always smaller for blinatumomab versus SOC, particularly in the high blasts group. Functioning status scores tended to stay the same or worsen with both blinatumomab and SOC regardless of blast level, except emotional scores, which improved with blinatumomab regardless of blast level (Figure 1). Symptom scores generally improved with blinatumomab but not with SOC, particularly in patients with high blasts (Figure 2). TTD analyses showed that hazard ratios favored blinatumomab over SOC, particularly in patients with high blasts (Table).
Conclusions: Blinatumomab improved HRQoL in patients with r/r Ph- BCP ALL and delayed the time to clinically meaningful deterioration in HRQoL compared with SOC. The treatment effects of blinatumomab versus SOC on HRQoL were particularly larger among patients with high disease burden.
Stein:Amgen Inc.: Speakers Bureau; Celgene: Speakers Bureau. Zimmerman:Amgen Inc.: Employment, Equity Ownership. Dombret:Novartis: Consultancy, Honoraria, Research Funding; Agios: Consultancy, Honoraria; Sunesis: Consultancy, Honoraria; Ambit (Daiichi Sankyo): Consultancy, Honoraria; Karyopharm: Consultancy, Honoraria; Menarini: Consultancy, Honoraria; Astellas: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Servier: Consultancy, Honoraria; Seattle Genetics: Consultancy, Honoraria; Cellectis: Consultancy, Honoraria, Other: Travel expenses; Celgene: Consultancy, Honoraria, Other: Travel expenses, Speakers Bureau; Immunogen: Consultancy, Honoraria; Shire-Baxalta: Consultancy, Honoraria; Abbvie: Consultancy, Honoraria; Otsuka: Consultancy, Honoraria; Kite Pharma: Consultancy, Honoraria, Research Funding; Jazz Pharma: Consultancy, Honoraria, Research Funding; Ariad (Incyte): Consultancy, Honoraria, Other: Travel expenses, Research Funding, Speakers Bureau; Roche/Genentech: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria, Research Funding, Speakers Bureau; Amgen: Consultancy, Honoraria, Other: Travel expenses, Research Funding, Speakers Bureau. Topp:F. Hoffmann-La Roche Ltd: Membership on an entity's Board of Directors or advisory committees, Research Funding; Regeneron Pharmaceuticals, Inc.: Honoraria, Research Funding; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel, Research Funding; Boehringer Ingelheim: Research Funding. Franklin:Amgen Inc.: Employment, Equity Ownership. Cong:Amgen, Inc.: Employment, Equity Ownership. Zhang:Amgen Inc.: Employment, Equity Ownership. Schuh:Pfizer: Consultancy; Novartis: Consultancy; Celgene: Consultancy; Teva: Consultancy; Amgen Inc.: Consultancy; Otsuka: Consultancy; Jazz: Consultancy; Shire: Consultancy.

